Health services use for transport injuries among children and youth in Ontario from 2015–2022: a population-based study
Abstract
Transportation-related injuries remain one of the leading causes of mortality among children and youth in Canada. Factors such as age, sex, marginalization, and the COVID-19 pandemic may influence children’s interactions with their environment and their mobility patterns. The objectives of this study were to describe: (1) the incidence of transport-related emergency department (ED) visits and hospitalizations in Ontario by type (motor vehicle, pedestrian, cycling) and by age and sex; and (2) the temporal trends in transport-related health service utilization by type and level of marginalization over time, including during the COVID-19 pandemic. Data for all traffic and non-traffic motor vehicle and vulnerable road user injuries (VRU, pedestrians and cyclists) were obtained for ED visits and hospitalizations in Ontario from January 2015 to March 2022. Descriptive analyses were completed by age group, sex, and marginalization across the study period. A simulation approach using Bayesian Poisson regression was employed to examine how the pandemic affected temporal trends. During the study period, the rate per 10 000 children and youth with motor vehicle-related injuries was 328 (95% CI: 325–331), and for VRU-related injuries was 275 (95% CI: 272.4–277). Sixty-one percent of cyclist ED visits and hospitalizations were non-traffic related. Males, children and youth aged 10–19 and more marginalized children generally had higher rates of both ED visits and hospitalizations than females, children aged 0–9 and those less marginalized. At the onset of the pandemic, ED visits for traffic-related motor vehicle and all pedestrians were lower than expected, and non-traffic motor vehicle and all cyclists were higher than expected. The greatest differences from expected in ED visits were in the least marginalized children; for example, there was a 107% increase in cyclist non-traffic in the least marginalized versus 11% increase in the most marginalized quintile. The findings of this study reinforce the ongoing need to focus on cycling safety, particularly non-traffic-related, for children and youth. These findings can also inform future equitable injury preventive efforts in light of significant population-level events, such as pandemics, that might change children’s mobility patterns.
1. Introduction
Transport-related injuries are a leading cause of child and youth (0-19 years) hospitalizations and death in Canada, with ~17,200 injuries/fatalities in 2023 alone (Transport Canada, 2023a). These injuries are a significant burden on the healthcare system, with costs totaling $284 million among children aged 0-14 years in 2018 (Parachute, 2021). On a positive note, there has been decrease observed in transportation injuries in children and youth in Canada over the past two decades (Fridman, Fraser-Thomas, Pike, & Macpherson, 2018; Rothman, Macarthur, Wilton, Howard, & Macpherson, 2019; Schwartz, Rothman, Howard, To, & Macarthur, 2022) which may be attributed to advancements in child safety seats, graduated licensing for teenagers and youths, improved vehicle designs and the adoption of the safe system approach in many jurisdictions (World Health Organization, 2023). According to the Transport Canada, National Collision Database (NCDB), transport injuries in children and youth ages 0-19 decreased 26% in the last 10 years from 2014 (23, 027) to 2023 (1,701), with a 5% drop in fatalities (Transport Canada, 2023b).
With the onset of the COVID-19 pandemic in March 2020 there were, however, substantial shifts in people’s mobility patterns which would have changed their exposure to traffic injury. According to the NCDB, in 2020, there were notable increases in pedestrian and decreases in motor vehicle collision (MVC) injuries and fatalities, with a small peak in cyclist injuries in 2021 (Transport Canada, 2023b). Policy responses to the COVID-19 pandemic, such as physical distancing and lockdown periods, may have influenced these trends by changing how people interacted with their environments (Tan, Wang, Xu, Zhang, & Luo, 2023). In Ontario, children and youth transportation patterns were influenced by multiple policies including stay-at-home orders, closures to schools, early childhood education centres, daycares, recreation and outdoor play spaces, and changes to the roadway-built environment to facilitate active transportation (i.e. walking and cycling, AT) (de Lannoy, Rhodes, Moore, Faulkner, & Tremblay, 2020; Szpunar et al., 2021).
1.1 Physical activity and transportation mode changes associated with the COVID-19 pandemic
Physical activity and transportation mode changes with the onset of the pandemic for children and youth were reported in Canada and internationally with varied findings.. Several studies showed decreases in physical activity and AT during the initial stages of the pandemic. A 2020 online Canadian national longitudinal survey and a cross-sectional survey of parents of children ages 5-17 conducted by ParticipACTION conducted early in the pandemic, reported decreases in AT of 37.5% and 35.7% respectively, with increases in screen and social media time during the epidemic (Larouche et al., 2022; Mitra et al., 2020; Moore et al., 2020). Results from the ParticipACTION survey found that a greater proportion of children and youth classified as low income. living in apartments, high density areas or close to a major roadway reported decreased outdoor activities (including AT) especially in children (Mitra et al., 2020; Moore et al., 2020). Another online qualitative study conducted across the U.S, found that families in the lower-income bracket had less access to outdoor space and subsequently those children had fewer opportunities to be physically active (Perez, Thalken, Ughelu, Knight, & Massey, 2021).
Other studies found differing results, with AT dropping more in higher income groups. In a survey conducted in Hanoi, Vietnam, AT dropped 22% (from 53% to 23%), with decreases higher in wealthier urban districts compared with poorer, non-urban districts (Nguyen, Pojani, Nguyen, & Ha, 2021). Families that owned cars or had mothers with work flexibility were more likely to shift from active school transportation to more motorized travel. In Western Australia, a community–based survey found that unstructured physical activity significantly increased, that is, outdoor play in the yard or the street near the house, park or playground areas, and indoor active play (Nathan et al., 2021); however this study did not consider socioeconomic status. A survey in Idaho, Washington and Oregon in the US conducted later on in the pandemic (2023) found no changes in active school transportation which was at approximately 14% (Chang, Xinyi, & Abdel-Rahim, 2024). The authors concluded that although there may have been short-term changes in school transportation mode, this was difficult to capture in a cross-sectional survey and modal changes may have bounced back to pre-pandemic modes as the pandemic progressed. However, this study did find that those more likely to report travel behaviour changes were children with more than one parent in the household, higher parent education level and higher household income suggesting that households with both the financial resources and education were more inclined to modify their children's school commuting behaviours (Chang et al., 2024). The inconsistencies in results across studies illustrate the importance of local context and the consideration of social marginalization factors when examining trends in physical activity and active transportation in children.
In addition to AT changes, there were differences in private car use during the pandemic. In Canada and internationally, there was a general shift from other transportation modes, including public transportation, towards personal car use, with some evidence that this shift has remained post-pandemic (Abdullah, Dias, Muley, & Shahin, 2020; Abouelela, Samir, & Antoniou, 2024; Ciuffini, Tengattini, & Bigazzi, 2023; Currie, Jain, & Aston, 2021; Haseeb & Mitra, 2024). In the initial phase of the pandemic, a survey conducted in six major Canadian metropolitan regions found that commuters used their personal cars significantly more with corresponding drops in public transit use (Labonté-LeMoyne, Chen, Coursaris, Sénécal, & Léger, 2020). In May 2023, over 80% of commuters in Canada used a personal vehicle, with an increase in the number of commuters across all provinces using a personal vehicle from 2021. These shifts to more private vehicle use could have implications for transportation injury for vehicle occupants, pedestrian and cyclists, with respect to changes in potential exposure (Statistics Canada, 2023).
1.2 Changes to transportation injuries associated with the COVID-19 pandemic
The transportation shifts with the onset of the pandemic may have affected trends in transportation injuries due to changes in potential exposure to traffic. In Canada, studies examining the impact of the pandemic on collision trends have been primarily focused on all ages or adults and did not focus specifically on children and youth. In Ontario, Canada for example, motor- and non-motor vehicle cycling injuries of all ages exceeded what was expected following the start of the COVID-19 pandemic, increasing by 13% and 47%, for emergency department (ED) visits and 46% and 50% for hospitalizations, respectively (Sammy et al., 2024). In Toronto, ED visits and hospitalizations of pedestrians decreased by 35% (95% CI: 28%, 42%) and 19% (95% CI: 2%, 32%), respectively, during the pandemic (Batomen et al., 2024). In Ontario, there was a 64.7% drop in collisions reported to the Ministry of Transportation involving drivers aged 80 years and over, and a 22.9% drop in those 35-54 years from the 30 days prior to the declaration of a state of emergency in Ontario on Marc 17, 2020 and the subsequent 30 days (Rapoport et al., 2021).
It is important, however; that health care utilization trends for transportation injuries in children and youth be examined independently, as trends may differ from those of adults due to the differing effects that pandemic policies may have had on their mobility. It is also important to consider social marginalization which may have important implications for these trends. Several international studies examined children’s ED visit trends over the COVID-19 pandemic in general and more specific to transport injury (Bernstine, Edelstein, & Krupik, 2023; Keays, Friedman, & Gagnon, 2020; Lazzerini et al., 2020). A common limitation of previous studies that examined ED visits and hospitalizations among children during the pandemic was that they did not analyze the trends by individual transportation modes (i.e., motor vehicle, cyclists, pedestrians), which is important to differentiate when mobility patterns change. In Italy, there was a significant decrease in pediatric ED visits for all causes (from 73% to 88%) during the pandemic compared to pre-pandemic times (Lazzerini et al., 2020). A study in Israel, found that the number of ED visits for injuries specifically, decreased during COVID-19 lockdowns compared to the pre-pandemic average among children aged 0-17 years, but this study did not distinguish between intentional and unintentional (e.g., transport-related) injuries (Bernstine et al., 2023). A study in Montréal reported significant decreases in motor vehicle collisions, sports-related injuries, and recreational ED visits (ranging from 35% among children aged 2-5 years old to an 83% decline among those aged 12–17 years) during the COVID-19 lockdown (Keays et al., 2020).
Research related to the number of transport-related hospitalizations remains underexplored, particularly in child and youth, as most studies have focused solely on ED visits. Hospitalization trends are important to examine as they represent the most severe injuries. Moreover, differences in transportation injury trends by demographic characteristics and socioeconomic status during the pandemic have also been underexplored. Understanding transport injury trends in health services use during the pandemic can provide important insights to inform preventive efforts and service use, in light of potential future events that may lead to changes in mobility. The objectives of this study, therefore, were to describe (1) the incidence of transport-related ED visits and hospitalizations by transportation type (motor vehicle, pedestrian, cycling) and by age and sex, (2) the temporal trends in transport-related ED visits and hospitalizations among children and youth by type and level of marginalization as related to the COVID-19 pandemic.
2. Methods
2.1 Study design
Jnjury trends were examined using an interrupted time series study design with March 17, 2020, the date of the Ontario Declaration of Emergency related to the COVID-19 pandemic-as the single interruption point (Government of Ontario, 2020).
2.2 Study population
The study population was children and youth between the ages of 0 and 19 years who experienced ED visits or hospitalizations in Ontario for transport injuries between 1 January 2015 and 31 March 2022. Those without a valid Ontario Health Insurance Plan (OHIP) number, residing outside Ontario at the time of injury, those with a repeat ED visit within seven days were excluded.
2.3 Data sources
ED visit and hospitalization data were extracted for children and youth ages 0-19 from the National Ambulatory Care Reporting System (NACRS) (Canadian Institute for Health Information (CIHI), 2023) and the Discharge Abstract Database (DAD) (Canadian Institue for Health Information (CIHI), 2023) from 1 January 2015 to 31 March 2022 (Canadian Institute for Health Information, n.d.-a). These data were obtained from ICES, a health services research organization funded by the Ontario Ministry of Health (IC/ES, 2025). The 2021 Ontario Marginalization Index (ON-Marg) was used as a measure of neighbourhood economic, ethno-racial, age-based, and social marginalization (Matheson, Dunn, Smith, Moineddin, & Glazier, 2012). This index includes four dimensions: households and dwellings, material resources, age and labour force, and racialized and newcomer populations. The focus of these analyses will be on the material resources dimension as a measure of marginalization, which is comprised of indicators related to access to and attainment of basic material needs.
2.4 Outcomes
The International Classification of Diseases (10th edition, adapted for Canada, ICD-10-CA) was used to extract all unintentional injury-coded cases. Data were extracted for traffic and non-traffic motor vehicle and vulnerable road user (VRU) ED visits and hospitalizations (pedestrians and cyclists). According to the ICD-10, traffic-related incidents are those occurring on a public highway, whereas a non-traffic incident occurs in places other than public highways (e.g. home, off-road). The codes are based on the external cause of injury reported in the hospital record which are used to identify the mechanism, intent and place/activity of an injury. We did not include other injury causes such as roadway falls. The sum of these injuries is referred to as transport-related injuries. Transport ICD-10-CA codes have been shown to have a high validity (positive predictive value = 96.5%) (Paleczny, Osagie, Sethi, & Cusimano, 2024). The codes used to extract data are summarized in Table 1.
For the descriptive analysis, incidence rates were calculated per 10,000 using extrapolated 2018 Canadian census population estimates for the total population, male and female, for ages 0-9 and 10-19 and by quintiles of marginalization as the midpoint of our data. The total census population equaled 3,033,083; with males-1,556.653, females- 1.476.430 and 0-9 years- 1.451.245, 10-19 years- 1.581,842. Outcomes for the temporal trend analysis were monthly ED visits and hospitalizations by transportation mode.
| Injury type | Mechanism | ICD-10 codes |
|---|---|---|
| Motor vehicle | traffic-related | [V02–V04](.1,.9), V09.2, [V12–V14](.3–.9), V19(.4–.6), [V20–V28](.3–.9), [ V29–V79](.4–.9), V80(.3–.5), V81.1, V82.1, [V83–V86](.0–.3), V87(.0–.8), V89.2 |
| non-traffic-related | [V20–V28](.0–.2), V29(.0-.3), [V30–V79](.0–.3), V81.0, V82.0, [V84-V85](.5–.9), V86(.4–.9), V88(.0–.8), V89.0 | |
| Cyclist | traffic-related | V104-V109, V114-V119, V124-V129, V134-V139, V144-V149, V154-V159, V164-V169, V174-V179, V184-V189, V194-V199 |
| non-traffic-related | V100-V102, V110-V112, V120-V122, V130-V132, V140-V142, V150-V152, V160-V162, V170-V172, V180-V182, V190-V193, [V103, V113, V123, V133, V143, V153, V163, V173, V183, V198] * | |
| Pedestrian | traffic-related | V011, V021, V031, V041, V051, V061, V092, V093 [V019, V029, V039, V049, V059, V069, V099] ** |
| non-traffic-related | V010, V020, V030, V040, V050, V060, V090, V091 |
2.5 Statistical analysis
2.5.1 Descriptive analysis
Incident rate ratios (IRR), with 95% confidence intervals were calculated and compared over a 7.25-year study period by age, sex, marginalization and ED visits and hospitalizations for total transport, traffic- and non-traffic-related motor vehicle and VRU injuries.
2.5.2 Trend analysis
A single interruption point was set at March 27, 2020, the date of the Ontario Declaration of Emergency related to the COVID-19 pandemic (Government of Ontario, 2020). A simulation approach was employed to examine how the pandemic affected injury trends. Monthly ED visits and hospitalizations were modelled using a Bayesian Poisson regression that included a first-order autoregressive term to account for autocorrelation. The model adjusted for month-specific seasonality and population size through an offset, and parameter estimation was calculated using Integrated Nested Laplace Approximation (INLA) (Brandt & Williams, 2001; Rue, Martino, & Chopin, 2009; White & Bennetts, 1996). The model was fit using pre-pandemic data (January 2015-December 2019) to forecast the expected number in the COVID=19 period, had the pandemic not occurred. The first quarter of 2020 was excluded from post-period calculations, as it was predominantly pre-pandemic. The mean difference in monthly outcome counts and the overall percent change, defined as observed-expected/expected, were calculated. The point estimates were the median values from the simulations, and the lower and upper bounds of the credible intervals (CI) were represented by the 2.25 and 97.75 percentiles, respectively. Trends by age and sex were analyzed for total transport injuries, as these data were unavailable by mode domain quintiles.
Interrupted time series (ITS) by individual modes were generated for ED visits; however, estimations for hospitalizations could not be completed by transportation mode due to the small sample size. Expected versus observed counts in the COVID-19 period were compared to determine whether the start of the pandemic affected transportation injury trends. The percent difference in ED visits between the observed monthly counts and the expected counts after March 2020, was also calculated for the ON-Marg material resources dimension quintiles. All analyses were performed in R version 4.4.2 (R Core Team, 2022).
3. Results
3.1 Descriptive analysis
During the study period, overall there were 69,617 motor vehicle (328.24/10 000, 95% CI: 325.46, 331.24) and 65,797 VRU (275.03/10 000, 95% CI: 272.39, 277.68) ED visits of which 49,684 (71%) and 41,617 (63%) respectively were prior to the pandemic (Table 2). Cyclists represented approximately 90% of VRU ED visits, with most of these (62.2%) being non-traffic-related. A smaller proportion of pedestrian ED visits were non-traffic-related (24.0%). Males showed significantly higher rates of ED visits for all modes, except for motor vehicle-traffic. The highest IRR comparing males to females for ED visits was for cyclists (IRR: 2.51, 95% CI: 2.43–2.58), with similar findings for traffic and non-traffic incidents. Individuals aged 10-19, compared to those aged 0-9, showed higher rates of ED visits, with the highest IRR being motor vehicle non-traffic visits (IRR: 4.52, 95% CI: 4.35–4:70), with pedestrian traffic incidents following closely (IRR: 4.09, 95% CI: 3.81–4.38). The most marginalized groups had higher rates compared with the least marginalized reference group, for motor vehicle and pedestrian ED visits, with the highest IRR for pedestrian traffic (IRR 2.1, 95% CI: 2.0-2.3) in the most marginalized group (Table 3).
There were overall 3,715 motor vehicle (2.46/10 000, 95% CI 2.38, 2. 53) and 2,435 VRU (1.61/10 000, 95% CI: 1.55, 1.67) hospitalizations, of which 2,714 (73%) and 1,375 (57%) respectively, were before the pandemic (Table 4). During the study period, VRUs overall accounted for approximately 40% of all transport hospitalizations. Cyclists represented 73% of VRU hospitalizations, with most of these (61%) being non-traffic related. A smaller proportion of pedestrian hospitalizations were non-traffic (23%). Males showed higher rates for hospitalizations than females for all modes, with the highest IRR for motor vehicle non-traffic (IRR: 3.83, 95% CI: 3.32–4.41), followed by cyclists overall (2.84, 95% CI 2.54–3.16). Individuals aged 10–19 compared to those aged 0–9 generally showed significantly higher rates of hospitalizations, except for pedestrian non-traffic (IRR: 0.77, 95% CI: 0.56–1.06), with the highest IRR being for motor vehicle non-traffic hospitalizations (IRR: 3.76, 95% CI: 3.26–4.23). Similar to ED visits, higher marginalized groups had higher rates for motor vehicle and pedestrian hospitalizations compared with the least marginalized group, with the exception of motor-vehicle non-traffic injuries (Table 5). Again, the highest IRR was for pedestrian traffic (IRR 2.3, 95% CI: 1.7-3.0) in the most marginalized group.
| Totals | Sex | IRR (95% CI) | Age | IRR (95% CI) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Rate/10 000 | Female | Rate/10 000 | 10-19 | Rate/10 000 | 0-9 | Rate/10 000 | |||||
| Total | 135 414 | 83 590 | 537 | 51 824 | 351 | 1.5 (1.5, 1.5) | 101 712 | 643 | 33 702 | 232 | 2.8 (2.7, 2.80) | |
| Motor Vehicle | Total | 69 617 | 37 311 | 240 | 32 306 | 219 | 1.1 (1.1, 1.1) | 57 122 | 361 | 12 495 | 86 | 4.2 (4.1, 4.3) |
| Traffic | 51 278 | 24 556 | 158 | 26 722 | 181 | 0.9 (0.9, 0.9) | 41 875 | 265 | 9 403 | 65 | 4.1 (4.0, 4.2) | |
| Non-traffic | 18 339 | 12 755 | 82 | 5 584 | 378 | 2.2 (2.1, 2.22) | 15 247 | 96 | 3 092 | 21 | 4.5 (4.4, 4.7) | |
| VRU | Total | 65 797 | 46 279 | 297 | 19 518 | 132 | 2.3 (2.2, 2.3) | 44 590 | 282 | 21 207 | 146 | 1.9 (1.9, 2.0) |
| Cyclist | Total | 58 903 | 42 643 | 274 | 16 260 | 110 | 2.5 (2.2, 2.5) | 39 288 | 248 | 19 615 | 135 | 1.8 (1.8, 1.9) |
| Traffic | 22 258 | 16 155 | 104 | 6 103 | 41 | 2.5 (2.4, 2.6) | 15 931 | 101 | 6 327 | 44 | 2.3 (2.2, 2.4) | |
| Non-traffic | 36 645 | 26 488 | 170 | 10 157 | 69 | 2.5 (2.4, 2.5) | 23 357 | 148 | 13 288 | 92 | 1.6 (1.6, 1.6) | |
| Pedestrian | Total | 6 894 | 3 636 | 23 | 3 258 | 22 | 1.1 (1.0, 1.1) | 5 302 | 33 | 1 592 | 11 | 3.1 (2.9, 3.2) |
| Traffic | 5 243 | 2 714 | 17 | 2 529 | 17 | 1.0 (1.0, 1.1) | 4 283 | 27 | 960 | 67 | 4.1 (3.8, 4.4) | |
| Non-traffic | 1 651 | 922 | 6 | 729 | 5 | 1.2 (1.1, 1.3) | 1 019 | 6.44 | 632 | 4 | 1.5 (1.3, 1.6) | |
| Totals | Least marginalized | Low marginalization | Moderate marginalization | High marginalization | Most marginalized | Missing | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Rate/ 10 000 | IRR (95% CI) | N | Rate/ 10 000 | IRR (95% CI) | N | Rate/ 10 000 | IRR (95% CI) | N | Rate/ 10 000 | IRR (95% CI) | N | Rate/ 10 000 | IRR (95% CI) | ||||
| Total | 135414 | 26544 | 433 | Ref | 29002 | 473 | 1.1 (1.1-1.1) | 26689 | 435 | 1.0 (1.0-1.0) | 23806 | 388 | 0.9 (0.9-0.9) | 26969 | 440 | 1.02 (1.00-1.03) | 2404 | |
| Motor Vehicle | Total | 69617 | 12396 | 202 | Ref | 14592 | 238 | 1.2 (1.2-1.2) | 14296 | 233 | 1.2 (1.1-1.2) | 12799 | 209 | 1.0 (1.0-1.1) | 14126 | 230 | 1.14 (1.11-1.17) | 1408 |
| Traffic | 51278 | 8890 | 145 | Ref | 10407 | 170 | 1.2 (1.1-1.2) | 10275 | 168 | 1.2 (1.1-1.2) | 9478 | 155 | 1.1 (1.0-1.1) | 11358 | 185 | 1.3 (1.2-1.3) | 870 | |
| Non-traffic | 18339 | 3506 | 57 | Ref | 4185 | 68 | 1.2 (1.1-1.3) | 4021 | 66 | 1.2 (1.1-1.2) | 3321 | 54 | 0.9 (0.9-0.9) | 2768 | 45 | 0.8 (0.7-0.8) | 538 | |
| VRU | Total | 65797 | 14148 | 231 | Ref | 14410 | 235 | 1.0 (0.9-1.0) | 12393 | 202 | 0.9 (0.8-0.9) | 11007 | 179 | 0.8 (0.8-0.8) | 12843 | 209 | 0.9 (0.9-0.9) | 996 |
| Cyclist | Total | 58903 | 13100 | 214 | Ref | 13248 | 216 | 1.0 (0.9-1.0) | 11175 | 182 | 0.9 (0.8-0.9) | 9673 | 158 | 0.7 (0.7-0.8) | 10821 | 176 | 0.8 (0.8-0.9) | 886 |
| Traffic | 22258 | 5123 | 84 | Ref | 4915 | 80 | 1.0 (0.9-1.0) | 4127 | 67 | 0.8 (0.8-0.8) | 3532 | 58 | 0.7 (0.6-0.7) | 4245 | 69 | 0.8 (0.8-0.9) | 316 | |
| Non-traffic | 36645 | 7977 | 130 | Ref | 8333 | 136 | 1.1 (1.0-1.1) | 7048 | 115 | 0.9 (0.9-0.9) | 6141 | 100 | 0.8 (0.7-0.8) | 6576 | 107 | 0.8 (0.8-0.9) | 570 | |
| Pedestrian | Total | 6894 | 1048 | 17 | Ref | 1162 | 19 | 1.1 (1.1-1.2) | 1218 | 20 | 1.2 (1.1-1.3) | 1334 | 22 | 1.3 (1.2-1.4) | 2022 | 33 | 1.9 (1.8-2.1) | 110 |
| Traffic | 5243 | 757 | 12 | Ref | 844 | 14 | 1.1 (1.0-1.2) | 931 | 15 | 1.2 (1.1-1.4) | 1012 | 16 | 1.3 (1.2-1.5) | 1615 | 26 | 2.1 (2.0-2.3) | 84 | |
| Non-traffic | 1651 | 291 | 5 | Ref | 318 | 5 | 1.1 (0.9-1.3) | 287 | 5 | 1.0 (0.8-1.2) | 322 | 5 | 1.1 (0.9-1.3) | 407 | 7 | 1.4 (1.2-1.6) | 26 | |
| Totals | Sex | Rate/ 10 000 | IRR (95% CI) | Age | IRR (95 % CI) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Rate/ 10 000 | Female | 10-19 | Rate/ 10 000 | 0-9 | Rate/ 10 000 | ||||||
| Total | 6 150 | 4 314 | 28 | 1 836 | 12 | 2.2 (2.1, 2.4) | 4 494 | 28 | 1 656 | 11 | 2.5 (2.4, 2.6) | |
| Motor Vehicle | Total | 3 715 | 2 576 | 17 | 1 139 | 8 | 2.2 (2.0, 2.3) | 2 958 | 19 | 757 | 5 | 3.6 (3.3, 3.9) |
| Traffic | 2 506 | 1 607 | 10 | 899 | 6 | 1.7 (1.6, 1.8) | 1 986 | 13 | 520 | 4 | 3.5 (3.2, 3.9) | |
| Non-traffic | 1 209 | 969 | 6 | 240 | 2 | 3.8 (3.3. 4.4) | 972 | 6 | 237 | 2 | 3.8 (3.3, 4.3) | |
| VRU | Total | 2 435 | 1 738 | 11 | 697 | 5 | 2.4 (2.2, 2.6) | 1 536 | 7 | 899 | 6 | 1.6 (1.4, 1.7) |
| Cyclist | Total | 1 773 | 1 329 | 9 | 444 | 3 | 2.8 (2.5, 3.2) | 1 094 | 7 | 679 | 5 | 1.5 (1.3, 1.6) |
| Traffic | 695 | 520 | 3 | 175 | 1 | 2.8 (2.4, 3.3) | 471 | 3 | 224 | 2 | 1.9 (1.6, 2.3) | |
| Non-traffic | 1 078 | 809 | 5 | 269 | 2 | 2.9 (2.5, 3.3) | 623 | 4 | 455 | 3 | 1.3 (1.1, 1.4) | |
| Pedestrian | Total | 662 | 409 | 3 | 253 | 2 | 1.5 (1.3, 1.8) | 442 | 3 | 220 | 2 | 1.8 (1.6, 2.2) |
| Traffic | 511 | 312 | 2 | 199 | 1 | 1.5 (1.2, 1.8) | 373 | 2 | 138 | 1 | 2.5 (2.0, 3.0) | |
| Non-traffic | 151 | 97 | 1 | 54 | 1 | 1.7 (1.2, 2.4) | 69 | 1 | 82 | 1 | 0.8 (0.56, 1.1) | |
| Totals | Least marginalized | Low marginalization | Moderate marginalization | High marginalization | Most marginalized | Missing | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Rate/ 10 000 | IRR (95% CI) | N | Rate/ 10 000 | IRR (95% CI) | N | Rate/ 10 000 | IRR (95% CI) | N | Rate/ 10 000 | IRR (95% CI) | N | Rate/ 10 000 | IRR (95% CI) | ||||
| Total | 6150 | 1149 | 19 | Ref | 1215 | 20 | 1.1 (1.0-1.2) | 1163 | 19 | 1.0 (0.9-1.1) | 1143 | 19 | 1.0 (0.9-1.1) | 1305 | 21 | 1.1 (1.1-1.2) | 175 | |
| Motor Vehicle | Total | 3715 | 684 | 11 | Ref | 729 | 12 | 1.1 (1.0-1.2) | 741 | 12 | 1.1 (1.0-1.2) | 690 | 11 | 1.0 (1.0-1.1) | 741 | 12 | 1.1 (1.0-1.2) | 130 |
| Traffic | 2506 | 421 | 7 | Ref | 456 | 7 | 1.1 (1.0-1.2) | 490 | 8 | 1.2 (1.1-1.3) | 484 | 8 | 1.2 (1.1-1.3) | 577 | 9 | 1.4 (1.2-1.6) | 78 | |
| Non-traffic | 1209 | 263 | 4 | Ref | 273 | 4 | 1.0 (0.9-1.2) | 251 | 4 | 1.0 (0.9-1.1) | 206 | 3 | 0.8 (0.7-0.9) | 164 | 3 | 0.6 (0.5-0.8) | 52 | |
| VRU | Total | 2435 | 465 | 8 | Ref | 486 | 8 | 1.0 (0.9-1.2) | 422 | 7 | 0.9 (0.8-1.0) | 453 | 7 | 1.0 (0.9-1.1) | 564 | 9 | 1.2 (1.1-1.4) | 45 |
| Cyclist | Total | 1773 | 368 | 6 | Ref | 372 | 6 | 1.0 (0.9-1.2) | 311 | 5 | 0.8 (0.7-0.9) | 315 | 5 | 0.9 (0.9-1.0) | 378 | 6 | 1.0 (0.9-1.2) | 29 |
| Traffic | 695 | 158 | 3 | Ref | 142 | 2 | 0.9 (0.7-1.1) | 114 | 2 | 0.7 (0.6-0.9) | 123 | 2 | 0.8 (0.6-0.9) | 148 | 2 | 0.9 (0.8-1.2) | 10 | |
| Non-traffic | 1078 | 210 | 3 | Ref | 230 | 4 | 1.1 (0.9-1.3) | 197 | 3 | 0.9 (0.8-1.1) | 192 | 3 | 0.9 (0.8-1.1) | 230 | 4 | 0.9 (0.8-1.1) | 19 | |
| Pedestrian | Total | 662 | 97 | 2 | Ref | 114 | 2 | 1.2 (0.9-1.5) | 111 | 2 | 1.2 (0.9-1.5) | 138 | 2 | 1.4 (1.1-1.9) | 186 | 3 | 1.9 (1.5-2.5) | 16 |
| Traffic | 511 | 70 | 1 | Ref | 89 | 1 | 1.3 (0.9-1.7) | 77 | 1 | 1.1 (0.8-1.5) | 102 | 2 | 1.5 (1.1-2.0) | 160 | 3 | 2.3 (1.7-3.0) | 13 | |
| Non-traffic | 151 | 27 | 0.4 | Ref | 25 | 0.4 | 0.9 (0.5-1.6) | 34 | 0.5 | 1.3 (0.8-2.1) | 36 | 0.5 | 1.3 (0.8-2.2) | 26 | 0.4 | 1.0 (0.6-1.6) | 3 | |
3.2 Temporal trends
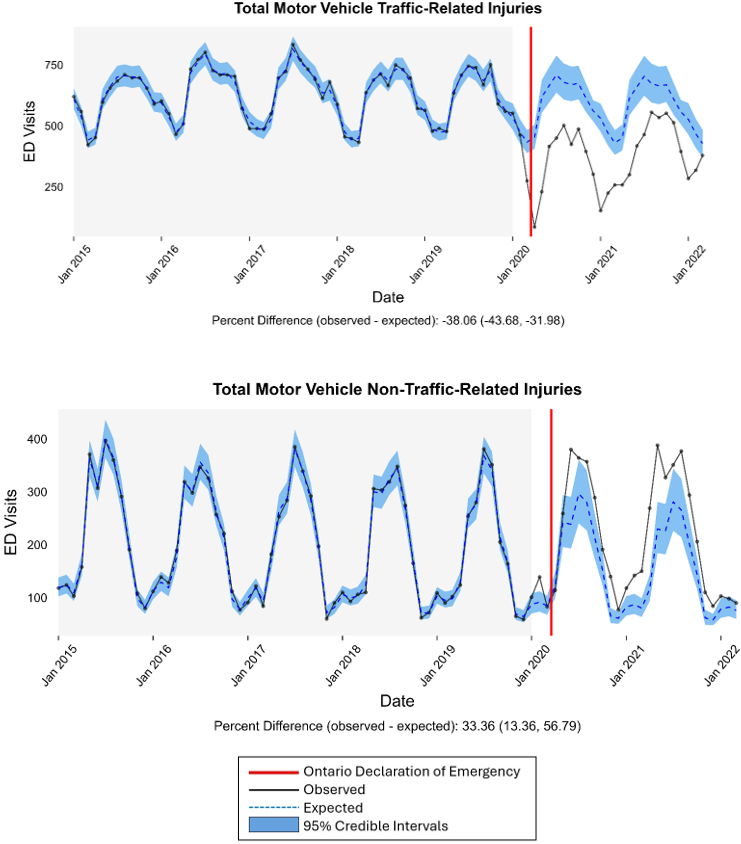
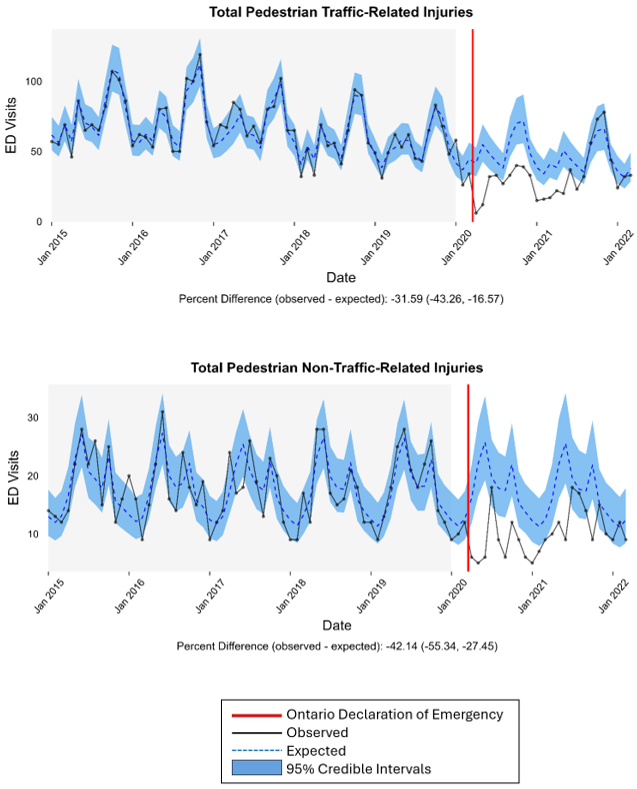
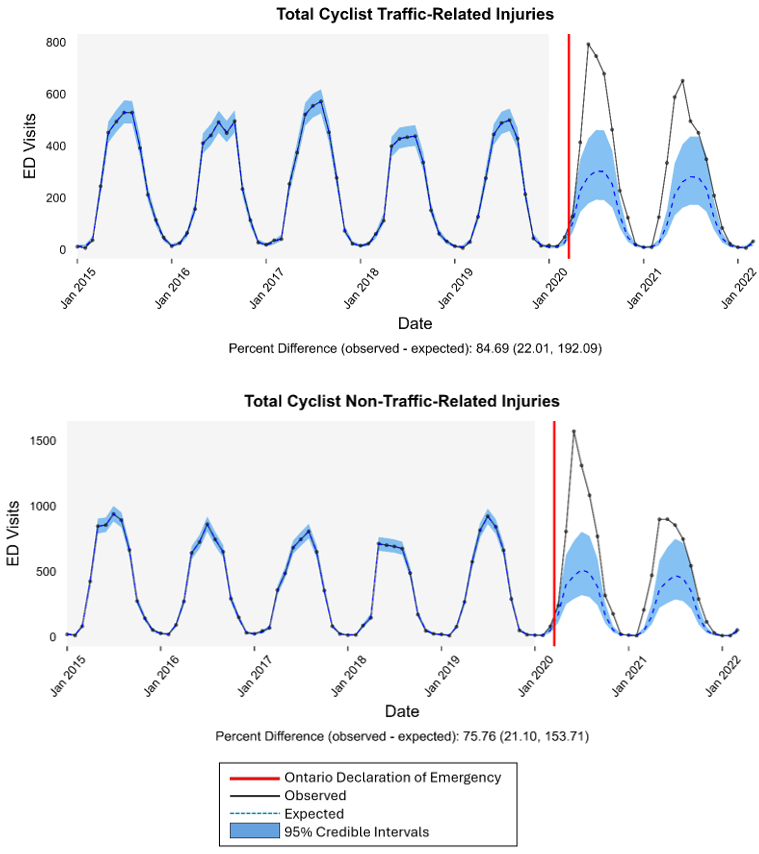
Monthly ED visits for traffic-motor vehicle and all pedestrians were lower than expected after the beginning of the pandemic, compared to pre-pandemic trends (Table 6). In contrast, monthly ED visits for non-traffic motor vehicle and all cyclists were higher. There were no significant differences in observed versus expected for overall transport ED visits and hospitalizations, or by sex or age after the start of the pandemic (trendlines not shown).
| ED visits | Hospitalizations | ||
|---|---|---|---|
| Transport-related | Total | 97.5 (-52.4, 218.3) | 12.0 (-3.5, 23.2) |
| Females | -46.9 (-106.2, 2.0) | 1.8 (-5.5, 6.8) | |
| Males | 130.3 (8.7, 225.0) | 9.7 (-3.4, 17.5) | |
| Age 0-9 y | -14.0 (-86.2, 44.5) | 2.5 (-7.0, 7.6) | |
| Age 10-19 y | 95.9 (-7.2, 185.4) | 9.7 (-2.6,18.51) | |
| Motor Vehicle | Traffic- | -242.5 (-306.0, -185.4) | |
| Non-traffic | 57.1 (26.5, 82.7) | ||
| Cyclist | Traffic | 139.8 (55.0, 200.5) | |
| Non-traffic | 221.6 (89.6, 311.5) | ||
| Pedestrian | Traffic | -16.2 (-26.8, -7.0) | |
| Non-traffic | -9.2 (-15.6, -4.8) |
Following the COVID-19 emergency declaration, there was a decrease in motor vehicle traffic-related ED visits (Figure 1). However, the number of motor vehicle non-traffic-related ED visits increased. There were similar decreases in all pedestrian ED visits (traffic and non-traffic) after the emergency declaration (Figure 2) and increases in all cycling ED visits (Figure 3). All trends returned to the expected level by the end of the study period.
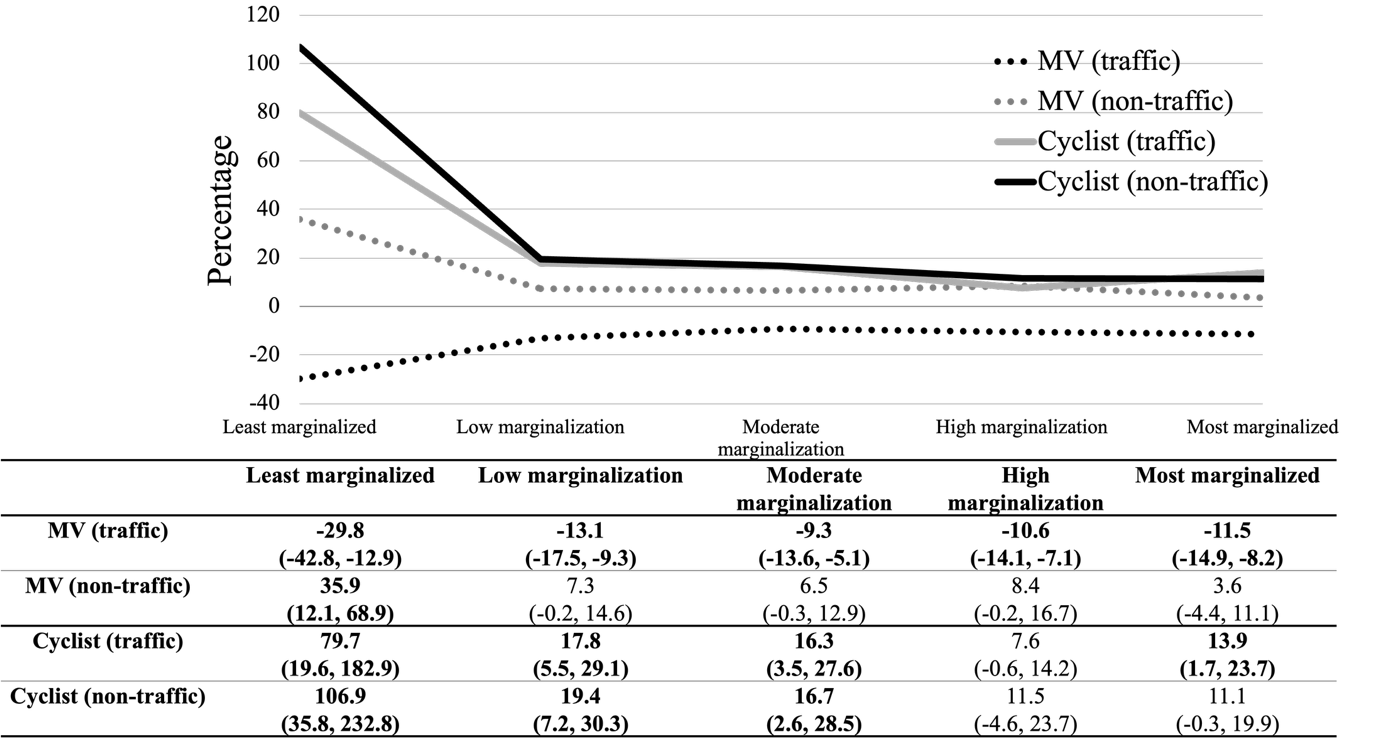
When examining different levels of neighbourhood marginalization, the greatest differences between observed and expected following the start of the pandemic, were in the least marginalized quintile (Figure 4). Estimates for pedestrian ED visits (traffic and non-traffic-related) were not reported due to small sample sizes.
4. Discussion
This study examined the incidence and temporal trends of transport-related ED visits and hospitalizations in Ontario by mode, age, sex, and level of marginalization. We found that the burden of transport ED visits for child and youth VRU was comparable to those motor-vehicle related. Notably, the majority of VRU ED visits and hospitalizations were cycling-related, and over 60% were non-traffic-related cycling ED visits and hospitalizations. Males, older and more marginalized children were generally more likely to experience transport-related ED visits and hospitalizations. The exception was cycling injuries where more marginalized children had lower rates ED visits and hospitalizations than the least marginalized children. Monthly ED visits for traffic-related motor vehicle and all pedestrians were lower than expected, and non-traffic motor vehicle and all cyclists were higher after the beginning of the pandemic, based on pre-pandemic trends; with no differences for transport hospitalizations overall or by age and sex. The least marginalized group of children appeared to be more sensitive to changes during the pandemic compared to the most marginalized, as indicated by greater differences in observed versus expected ED visits after the emergency declaration.
Previous studies show mixed findings regarding the preponderance of cycling injuries as compared with pedestrian injuries in health services data. Using the same data sources in Ontario from 2012 to 2021, but for all ages, our previous study found that cyclist health care visits were also substantially higher than pedestrians, with cyclist ED visits three times greater than pedestrian visits and almost six times greater for hospitalizations (Macpherson et al., 2024). Conversely, between 2015 and 2019 in British Columbia, all-ages pedestrian hospital admissions were three times higher than those of cyclists (Branion-Calles et al., 2025a) . This study included only on-road injuries as a result of interactions with motor vehicles, falls, and unknown causes. Another study using a national U.S. sample of 0–19-year-olds from 2006 to 2012, examining just motor vehicle-related injuries, also found that pedestrians represented the majority (73%) of pedestrian and cycling motor vehicle-related injuries (Wheeler-Martin, Mooney, Lee, Rundle, & DiMaggio, 2017). These contradictory results may be due to differing case definitions, with some studies looking at traffic and non-traffic, and others with and without the involvement of motor vehicles. This difference points to the importance of using the appropriate case definitions to address study objectives and to confirm case definitions when doing cross-study comparison. The results might also suggest that the type of VRU burden varies by location. Ontario, British Columbia, and a US national sample represent very different road environments in, for example, cycling infrastructure and motor vehicle traffic volumes and speeds. Different jurisdictions also may have different laws and policies related to, for example, helmets and distracted driving.
Although we found that the majority of VRU ED visits for child cyclists were non-traffic related, we did not find similar results for child pedestrians. As early as 1999, Stutts & Hunter noted that the majority of all-age cycling ED visits did not involve a motor vehicle (70%) when including all ages traffic and non-traffic injuries in the US (Stutts & Hunter, 1999). Brannion-Calles et al. (2025) found that close to 50% of all-age cycling hospital admissions were due to falls, 1.8 times more than motor vehicle injuries, and 20% with an unknown mechanism (Branion-Calles et al., 2025b). This study also found that 69% of pedestrian hospital admission injuries were due to falls, 2.3 times greater than those involving a motor vehicle. These findings reinforce the importance of considering case definitions, as our results may be different, as our analysis was limited to children and youth, versus other studies, which included all ages. Generally, however, all findings highlight the importance of including injuries sustained due to falls on roadways and off-road conditions, as well as a result of a on-road motor vehicle interaction.
Older children, males and more marginalized children were generally more likely to experience transport-related injuries related to ED visits and hospitalizations, with two exceptions: traffic-related motor vehicle ED visit injuries, where females experienced higher rates than males, and hospitalizations due to non-traffic-related pedestrian injuries, where no statistically significant difference was observed between age groups. Our results that indicated older children and youth and males have a higher risk of transport injuries, support findings of previous studies (Mannocci, Saulle, Villari, & La Torre, 2019; Peden et al., 2022; Swedler et al., 2024). Older children and youth may experience higher risk due to immaturity and low impulse control, their emerging independence to travel without supervision, and inexperience with traffic and potential substance abuse (Hammig & Davis, 2022; Spirito, Rasile, Vinnick, Jelalian, & Arrigan, 1997; Twisk, Bos, & Weijermars, 2017). However, we found that there were two exceptions to the general finding of higher risk for males; there were no differences in hospitalizations due to non-traffic-related pedestrian injuries between the sexes, and females experienced higher rates of traffic-related motor vehicle ED visits. Research consistently shows that women have a greater rate of severe injury and fatality in motor vehicle collisions (Abrams & Bass, 2024; Evans, 2000; Kahane, 2013). This may be due to anatomical and physiological differences, and the result of vehicle design issues (Abrams & Bass, 2024; Ryan et al., 2020). The development and use of female-specific crash test dummies is still evolving, and male crash dummies still tend to be the norm (Ryan et al., 2020).
The finding that more marginalized children had higher rates of transport-related injuries than less marginalized children has been well supported by previous research (Birken, Parkin, To, & Macarthur, 2006; Laflamme & Diderichsen, 2000; Rothman et al., 2017; Rothman et al., 2019; Naomi Schwartz et al., 2022). There is some evidence that differences in road traffic environments, with more marginalized areas having fewer road safety features and higher speed roadways, may contribute to this inequity (Rothman, Cloutier, et al., 2020). It appears that there is some discrepancy related to the risk of bicyclist injury in more marginalized children, with some studies indicating a higher risk as opposed to our study which found a lower risk (Carlin, Taylor, & Nolan, 1995; Embree, Romanow, Djerboua, Bourdeaux, & Hagel, 2016; Gagné & Hamel, 2009). This points to the importance of local context, as there are different road safety and cycling infrastructure in different cities, with potentially different access to bicycles.
The result of the trend analyses indicated that ED visits were more sensitive than hospitalizations to pandemic-related changes. We found that there were substantial decreases in motor vehicle-related and pedestrian ED visits after the state of emergency was declared, which returned to expected values by the end of the study period. However, the ED visits related to cycling increased during the pandemic. These results may be linked to changes in children’s exposure to traffic and mobility patterns because of school and daycare closures and stay-at-home orders, with more children cycling for recreation, and an increase in the number of novice cyclists. Previous research has found that cycling to school is rare, for example, in Toronto schools, with 61% of children walking and 2 % of children cycling (Rothman et al., 2021). Hospitalizations for transport injuries, however, remained consistent throughout the study period except for a slight decrease in the initial phases of the pandemic. Declines in visits to the ED likely reflected hesitancy to go to the hospital for more minor injuries during a pandemic, whereas more severe injuries necessitated a hospital visit (Boserup, McKenney, & Elkbuli, 2020; Kwok, Clapham, & Calder-Sprackman, 2021).
The marginalization analysis indicated that the least marginalized group was more sensitive to changes due to the pandemic related to ED visits for transportation injuries than the more marginalized groups. It is suggested that activities changed more for the less marginalized children, as they generally have more engagement in extra-curricular activities, which were cancelled during the pandemic, resulting perhaps in less motor vehicle travel (Richmond et al., 2022). Less marginalized children are also likely to have more opportunities for cycling due to affordability and living in more cycling-friendly environments than more marginalized children.
This study has several strengths and limitations. The strength is that it was a large population-based study using routinely collected health service and census data and, therefore, may be less subject to bias than single-study research. However, the inability to assess children’s exposure to the different modes of transportation and the changes in exposure due to the pandemic was a limitation. The relatively low number of child pedestrian injuries limited our ability to evaluate changes in pedestrian injuries by marginalization. Other Canadian studies have shown that children in poorer areas are more likely to suffer pedestrian injuries (Cloutier et al., 2017; Rothman, Fridman, Cloutier, Manaugh, & Howard, 2020; Rothman et al., 2019; Naomi Schwartz et al., 2022).
5. Implications
The results have several important implications for public health, transportation safety, health equity, and policymaking. Understanding the burden of injury and the injury trends by transportation mode, age, sex, and marginalization can provide essential insights to inform future injury preventive efforts, considering significant population-level events, such as pandemics, that might change children’s mobility patterns. First, interventions directed at VRU injury among children must be equity-informed, ensuring safe recreational and commuting options across sex and age and all marginalization levels.
Second, there is a need for injury prevention strategies and policies to focus on cycling safety, not solely on reducing interactions with cars, but also on preventing falls and on off-road infrastructure in parks and trails where many children ride, particularly as they get older and gain more independent mobility. Appropriate surveillance of these injuries must use health services data, as typically municipalities use police-reported data to monitor transport injuries, and police do not generally attend injuries not involving a motor vehicle or off-road. This also points to the need for cities to focus on developing safe cycling infrastructure for all ages, not only on-road but also off-road.
Third, the pandemic led to a decrease in pedestrian injuries, and an increase in cycling injuries, which indicates a need for awareness regarding the potential effects of future events that may lead to changes in child mobility, including a possible shift of regular commuting to school patterns (usually by walking) to more recreational mobility which may include more cycling and more novice riders. In addition, the observed drop in ED visits emphasized that the injury burden may be underrepresented during a pandemic, but the consistency in injury hospitalizations highlights the need for consistent trauma care capacity even during a public health emergency where there may be pressure to redirect resources elsewhere.
6. Conclusion
These findings provided a picture of variability in child and youth transport ED visits and hospitalizations, and the effects of a pandemic that influenced mobility patterns. The results highlight the need for road safety infrastructure that can adapt to changing patterns of children’s (and the population as a whole) mobility in the future. This work also highlights the importance of safe infrastructure addressing non-motor vehicle cycling injuries, as well as the continued surveillance of injuries and adequate healthcare during potential disruptive events in the future.
CRediT contribution
Linda Rothman: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft. Ian Pike: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing. Adrian Sammy: Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Visualization, Writing – review & editing. Saroar Zubair: Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – review & editing. Alex Zheng: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – review & editing. Shazya Karmali: Funding acquisition, Investigation, Methodology, Project administration, Writing – review & editing. Brice Batomen: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – review & editing. Andrew Howard: Formal analysis, Funding acquisition, Investigation, Methodology, Supervision, Writing – review & editing. Natasha Saunders: Funding acquisition, Investigation, Methodology, Resources, Writing – review & editing. Shelina Babul: Funding acquisition, Investigation, Methodology, Resources, Writing – review & editing. Omidreza Sadrmanesh: Investigation, Visualization, Writing – original draft. Fahra Rajabali: Funding acquisition, Investigation, Methodology, Writing – review & editing. Pamela Fuselli: Funding acquisition, Investigation, Methodology, Writing – review & editing. Alison K. Macpherson: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft.
Acknowledgements
This study was supported by ICES, which is funded in part by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study was based on data compiled by ICES. However, the analyses, opinions, and statements expressed herein are those of the authors and not necessarily those of ICES no endorsement is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by CIHI. However, the analyses, conclusions, opinions, and statements expressed in the material are those of the authors, and not necessarily those of CIHI. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and information compiled and provided by the Ontario Ministry of Health. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. We thank the Toronto Community Health Profiles Partnership for providing access to the Ontario Marginalization Index.
Declaration of competing interests
The authors have no conflicts to disclose.
Declaration of generative AI use
The authors declare that no generative AI was used in this work.
Prior dissemination declaration
An earlier version of this paper was presented at the CARSP/ICTCT conference, held in Québec city, Canada, on 20–23 May 2025.
Ethics statement
This study has been approved by the University of British Columbia, Children’s & Women’s Health Centre REB (H22-00166) and the Toronto Metropolitan University REB (REB 2022-106).
Funding statement
This research was funded by an operating grant from the Canadian Institutes of Health Research (UIP-179228XX).
Editorial information
Handling editor: Nicolas Saunier, Polytechnique Montréal, Canada.
Reviewer: Désirée Hagmann, Zurich University of Applied Sciences (ZHAW), Switzerland.
Submitted: 28 August 2025; Accepted: 25 May 2026; Published: 5 June 2026.